
- 首页 > 正文
ERA大咖谈丨Ⅲ期VALIANT试验52周数据揭晓:加速补体抑制疗法革新
发表时间:2025-08-19 14:57:57
编者按:在第62届欧洲肾脏协会(ERA)年会上,瑞士洛桑大学附属医院(CHUV)肾脏病学教授Fadi Fakhouri博士聚焦补体抑制疗法及其在C3肾小球病(C3G)和原发性免疫复合物膜增生性肾小球肾炎(IC-MPGN)中的应用进行学术报告,揭示了临床需要多种补体抑制剂的核心逻辑,并分享了Pegcetacoplan治疗C3G和原发性(特发性)IC-MPGN的Ⅲ期VALIANT试验的52周结果详细数据。肾医线就此话题对Fadi Fakhouri博士进行了专访,本文整理Fadi Fakhouri博士的大会报告及采访的主要内容,与广大肾脏病医生共享。
一、补体系统复杂性驱动多样化治疗需求
“补体系统包含40余种蛋白质,通过经典、凝集素和替代三条途径激活,不同肾脏疾病中补体的致病机制差异显著。”Fakhouri指出,“炎症性损伤多由C5激活介导,而C3G的关键驱动因素是C3沉积”。这种机制异质性要求治疗必须“精准靶向”——例如针对替代途径失调的C3G,需特异性抑制C3转化酶,而炎症为主的疾病则需靶向C5。此外,同一患者在疾病不同阶段的补体活化模式可能动态变化,进一步凸显了多样化抑制剂的必要性。
他以图表展示补体系统级联反应(图1):经典途径从C1复合物启动,替代途径依赖C3b与B因子结合,而终末途径共同形成膜攻击复合物(MAC)。“就像交响乐团需要不同乐器协作,补体系统的精密平衡一旦打破,就需要不同‘调节器’来纠正。”他强调,这种复杂性也体现在临床——约50%~80%的C3G患者存在C3肾炎因子,4%~12%携带抗H因子抗体(Kidney Int. 2020 Nov;98(5):1135-1148.),不同抗体亚型对应不同的治疗靶点。
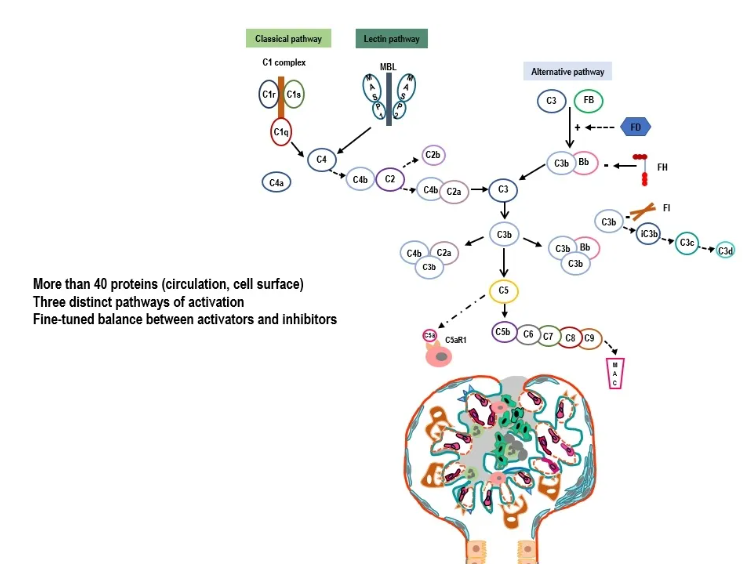
图1. 复杂的补体系统
Nephrology On-line: Your presentations highlight the evolving role of complement inhibition in treating C3G and primary IC-MPGN. Could you explain why multiple different complement inhibitors are needed in clinical practice?
Dr Fakhouri: As you know, the complement system is very complex, and even the involvement of complement in different kidney diseases relies on different molecules in the complement system. So, we need different therapeutic targets. For example, inflammation is more mediated by C5 activation. Whereas in C3G, the main driver is C3 deposition. So, you have different mechanisms of injury to the kidney due to complement, and we need to target each one specifically depending on the context of the disease, even sometimes, depending on the course of the disease, over time in a single patient.
二、VALIANT试验:补体抑制的长期疗效验证
针对Pegcetacoplan(培西他普)的Ⅲ期VALIANT试验数据成为本次报告的焦点。该试验为随机前瞻性试验,旨在评估Pegcetacoplan在青少年和成人C3G及免疫复合物性疾病患者中的疗效,共纳入124例患者。
在报告中,Fakhouri教授展示了治疗前后的肾活检对比:基线时弥漫性C3c阳性的肾小球,在26周的Pegcetacoplan治疗后转为阴性。机制上,该药物通过抑制C3转化酶,阻断C3b生成及下游炎症级联,从而减少肾小球损伤。试验还证实,治疗26周时,无论患者年龄(12岁以上)、疾病类型(C3G或IC-MPGN)、移植状态或基线蛋白尿水平,疗效均一致。例如,基线蛋白尿≥3 g/g的患者治疗后蛋白尿减少72.1%,合并免疫抑制剂治疗的患者也获得70.3%的降幅。
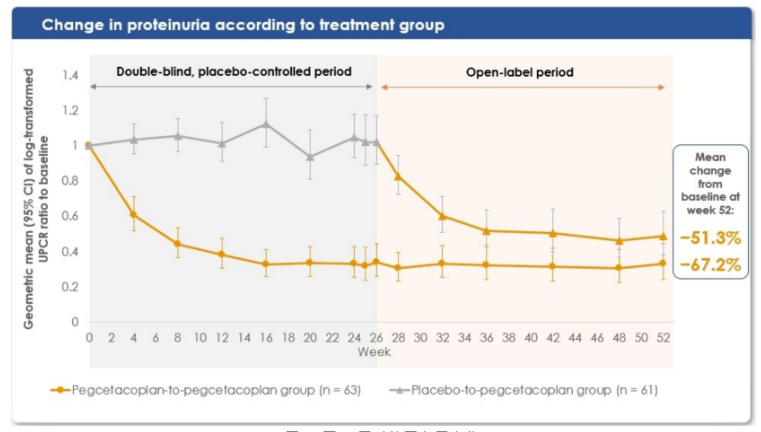
治疗52周(1年)时的结果显示,无论是初始即接受治疗还是6个月后从安慰剂转用Pegcetacoplan的患者,蛋白尿分别减少51%和67%(图2)——这种降幅在肾小球疾病中极为罕见。更值得关注的是,71%的患者在26周重复肾活检中显示C3c沉积完全清除,“传统治疗中,C3沉积的逆转几乎难以想象。”C3c 沉积的逆转是C3G和IC-MPGN患者疗效的关键标志。
此外,估算肾小球滤过率(eGFR)在一年内保持稳定。安慰剂组在初始六个月内 eGFR 有下降趋势,但转为Pegcetacoplan治疗后,肾功能有所恢复,最终 eGFR 与初始即接受治疗的患者相似。基于蛋白尿减少、肾脏C3c清除和 eGFR 早期稳定,VALIANT试验的这些结果令人瞩目。
图片
图2. 至52周时的蛋白尿变化
安全性方面,药物相关不良事件多为轻度输液反应,未出现脑膜炎球菌感染等严重并发症,长期使用的安全性与短期数据一致。这为临床提供了重要参考:Pegcetacoplan不仅疗效显著,且可避免糖皮质激素的副作用,尤其适用于需长期治疗的患者。
Nephrology On-line: The VALIANT trial with pegcetacoplan has shown sustained efficacy over 52 weeks in patients with C3G and IC-MPGN. What are the key clinical implications of these results for patients and clinicians?
Dr Fakhouri: The VALIANT study was a randomized prospective trial assessing the efficacy of pegcetacoplan in C3 glomerulopathy (C3G) and immune complex in adolescent and adult patients. After six months, all the placebo group was switched to pegcetacoplan. Here, we present the data at 52 weeks, one year, that are impressive. To make it simple for you, I'm going to give you just three figures – 51-67%0% reduction in proteinuria in patients who were from the beginning on pegcetacoplan and patients switched from placebo to pegcetacoplan, respectively; Such reduction in proteinuria is rarely seen in glomerular diseases. Besides, 71% of patients clearing all their C3c deposits in the kidney at a repeat kidney biopsy at 26 weeks (which is in my point of view a very impressive finding, because we are not very accustomed to seeing that);. The reversal of C3c deposits is a key finding of efficacy in C3G patients and immune complex-mediated membranoproliferative glomerulonephritis (IC-MPGN) patients. The short finding is that you have a stabilization of eGFR over one year. The placebo group tended to decrease in the initial six months, and then when they were switched to pegcetacoplan, they regained some renal function and, at the end, the eGFR was similar to those patients treated from the beginning with pegcetacoplan. Very impressive results based on proteinuria reduction, C3c removal from the kidney, and stabilization of eGFR as early as one year.
Fakhouri教授指出:“当前,我们正处于快速变革的时代,补体抑制剂将在不同适应证中找到定位。”面对补体介导性肾病的治疗前景,Fakhouri教授勾勒出清晰的发展蓝图:
抗炎药物的迭代升级:C5抑制剂有望取代糖皮质激素,成为炎症性肾病的一线选择。“患者可以告别激素导致的骨质疏松、感染风险,同时获得更持久的肾脏缓解。”
精准靶向治疗的普及:从“一刀切”的全身性抑制转向精准调控。例如,替代途径异常的C3G患者可靶向C3转化酶,而经典途径激活为主的疾病则需抑制C1复合物。这种“病理机制导向”的治疗模式将大幅提升疗效。
可及性与成本优化:随着更多企业入局补体领域以及更多补体药物上市,药物价格有望下降。竞争将推动技术创新,促进药物价格下降,使全球患者有能力负担并获得治疗。
Nephrology On-line: How do you envision the treatment paradigm for complement-mediated kidney diseases evolving in the next 5 to 10 years, and what research questions are most urgent to address?
Dr Fakhouri: This is a very excellent question, because I think we are living in very changing, moving times and complement inhibitors will find their place in different indications. For example, I see in the future that C5 inhibitors will replace corticosteroids sooner or later as anti-inflammatory drugs in inflammatory kidney disease. This would be a great change for doctors, but especially for patients. They could be spared the side effects of corticosteroids while achieving potentially a better renal remission. The second change I see is that we are moving towards a more targeted, specific pathogenesis-based approach to disease, where if you have an alternative pathway dysregulated, you have to target the alternative pathway. So, we are moving towards a fine-tuned, precise inhibition of the complement system, not a global inhibition like we had initially with C5 inhibition. And the third trend I see is a decrease in price due to the increase in the number of drugs and companies involved in the complement field, which would be good news for patients because decrease in price would make it more affordable and more easily available for patients worldwide.
四、补体领域:下一个肾脏病学革新前沿
“两三年前,SGLT2抑制剂和GLP-1受体激动剂引领了代谢性肾病的突破;如今,补体抑制正在开启新的治疗纪元。”Fakhouri在访谈中感慨。在ERA年会的众多议题中,补体抑制专场无疑成为焦点。从基础研究到临床转化的加速,将让补体靶向治疗成为继免疫抑制剂之后的又一里程碑。
Nephrology On-line: You have probably given a lot of talks, also joined a lot of sessions. Have you seen any sessions that you think are particularly interesting?
Dr Fakhouri: I think the complement inhibition is making a great revolution. Two or three years ago, we had the SGLT2 inhibitors and GLP-1 receptor agonists emerging into the light, and now it is time for complement inhibition. That is why I'm very happy to be here.
总结及展望
肾脏疾病治疗的范式正发生重要变革,尤其是补体治疗领域。除Pegcetacoplan外,针对C5、C1q、H因子等靶点的抑制剂已进入不同研发阶段,形成覆盖补体全通路的治疗矩阵。这不是单一药物的胜利,而是整个领域对疾病机制深入理解的成果。随着精准医学和人工智能在生物标志物发现中的应用,补体抑制疗法将进一步个性化,为终末期肾病的预防带来希望。
未来肾脏疾病的诊断不仅要依赖肾活检,更要结合血液和尿液中的补体活化标志物,如 C3a、C5a,实现疗效的动态监测。” 此外,如何确定最佳治疗疗程、筛选能安全停药的患者,以及探索补体抑制剂与其他靶向药物的联合方案,都是亟待解决的课题。
一、补体系统复杂性驱动多样化治疗需求
“补体系统包含40余种蛋白质,通过经典、凝集素和替代三条途径激活,不同肾脏疾病中补体的致病机制差异显著。”Fakhouri指出,“炎症性损伤多由C5激活介导,而C3G的关键驱动因素是C3沉积”。这种机制异质性要求治疗必须“精准靶向”——例如针对替代途径失调的C3G,需特异性抑制C3转化酶,而炎症为主的疾病则需靶向C5。此外,同一患者在疾病不同阶段的补体活化模式可能动态变化,进一步凸显了多样化抑制剂的必要性。
他以图表展示补体系统级联反应(图1):经典途径从C1复合物启动,替代途径依赖C3b与B因子结合,而终末途径共同形成膜攻击复合物(MAC)。“就像交响乐团需要不同乐器协作,补体系统的精密平衡一旦打破,就需要不同‘调节器’来纠正。”他强调,这种复杂性也体现在临床——约50%~80%的C3G患者存在C3肾炎因子,4%~12%携带抗H因子抗体(Kidney Int. 2020 Nov;98(5):1135-1148.),不同抗体亚型对应不同的治疗靶点。
图1. 复杂的补体系统
Nephrology On-line: Your presentations highlight the evolving role of complement inhibition in treating C3G and primary IC-MPGN. Could you explain why multiple different complement inhibitors are needed in clinical practice?
Dr Fakhouri: As you know, the complement system is very complex, and even the involvement of complement in different kidney diseases relies on different molecules in the complement system. So, we need different therapeutic targets. For example, inflammation is more mediated by C5 activation. Whereas in C3G, the main driver is C3 deposition. So, you have different mechanisms of injury to the kidney due to complement, and we need to target each one specifically depending on the context of the disease, even sometimes, depending on the course of the disease, over time in a single patient.
二、VALIANT试验:补体抑制的长期疗效验证
针对Pegcetacoplan(培西他普)的Ⅲ期VALIANT试验数据成为本次报告的焦点。该试验为随机前瞻性试验,旨在评估Pegcetacoplan在青少年和成人C3G及免疫复合物性疾病患者中的疗效,共纳入124例患者。
在报告中,Fakhouri教授展示了治疗前后的肾活检对比:基线时弥漫性C3c阳性的肾小球,在26周的Pegcetacoplan治疗后转为阴性。机制上,该药物通过抑制C3转化酶,阻断C3b生成及下游炎症级联,从而减少肾小球损伤。试验还证实,治疗26周时,无论患者年龄(12岁以上)、疾病类型(C3G或IC-MPGN)、移植状态或基线蛋白尿水平,疗效均一致。例如,基线蛋白尿≥3 g/g的患者治疗后蛋白尿减少72.1%,合并免疫抑制剂治疗的患者也获得70.3%的降幅。
治疗52周(1年)时的结果显示,无论是初始即接受治疗还是6个月后从安慰剂转用Pegcetacoplan的患者,蛋白尿分别减少51%和67%(图2)——这种降幅在肾小球疾病中极为罕见。更值得关注的是,71%的患者在26周重复肾活检中显示C3c沉积完全清除,“传统治疗中,C3沉积的逆转几乎难以想象。”C3c 沉积的逆转是C3G和IC-MPGN患者疗效的关键标志。
此外,估算肾小球滤过率(eGFR)在一年内保持稳定。安慰剂组在初始六个月内 eGFR 有下降趋势,但转为Pegcetacoplan治疗后,肾功能有所恢复,最终 eGFR 与初始即接受治疗的患者相似。基于蛋白尿减少、肾脏C3c清除和 eGFR 早期稳定,VALIANT试验的这些结果令人瞩目。
图片
图2. 至52周时的蛋白尿变化
安全性方面,药物相关不良事件多为轻度输液反应,未出现脑膜炎球菌感染等严重并发症,长期使用的安全性与短期数据一致。这为临床提供了重要参考:Pegcetacoplan不仅疗效显著,且可避免糖皮质激素的副作用,尤其适用于需长期治疗的患者。
Nephrology On-line: The VALIANT trial with pegcetacoplan has shown sustained efficacy over 52 weeks in patients with C3G and IC-MPGN. What are the key clinical implications of these results for patients and clinicians?
Dr Fakhouri: The VALIANT study was a randomized prospective trial assessing the efficacy of pegcetacoplan in C3 glomerulopathy (C3G) and immune complex in adolescent and adult patients. After six months, all the placebo group was switched to pegcetacoplan. Here, we present the data at 52 weeks, one year, that are impressive. To make it simple for you, I'm going to give you just three figures – 51-67%0% reduction in proteinuria in patients who were from the beginning on pegcetacoplan and patients switched from placebo to pegcetacoplan, respectively; Such reduction in proteinuria is rarely seen in glomerular diseases. Besides, 71% of patients clearing all their C3c deposits in the kidney at a repeat kidney biopsy at 26 weeks (which is in my point of view a very impressive finding, because we are not very accustomed to seeing that);. The reversal of C3c deposits is a key finding of efficacy in C3G patients and immune complex-mediated membranoproliferative glomerulonephritis (IC-MPGN) patients. The short finding is that you have a stabilization of eGFR over one year. The placebo group tended to decrease in the initial six months, and then when they were switched to pegcetacoplan, they regained some renal function and, at the end, the eGFR was similar to those patients treated from the beginning with pegcetacoplan. Very impressive results based on proteinuria reduction, C3c removal from the kidney, and stabilization of eGFR as early as one year.
Fakhouri教授指出:“当前,我们正处于快速变革的时代,补体抑制剂将在不同适应证中找到定位。”面对补体介导性肾病的治疗前景,Fakhouri教授勾勒出清晰的发展蓝图:
抗炎药物的迭代升级:C5抑制剂有望取代糖皮质激素,成为炎症性肾病的一线选择。“患者可以告别激素导致的骨质疏松、感染风险,同时获得更持久的肾脏缓解。”
精准靶向治疗的普及:从“一刀切”的全身性抑制转向精准调控。例如,替代途径异常的C3G患者可靶向C3转化酶,而经典途径激活为主的疾病则需抑制C1复合物。这种“病理机制导向”的治疗模式将大幅提升疗效。
可及性与成本优化:随着更多企业入局补体领域以及更多补体药物上市,药物价格有望下降。竞争将推动技术创新,促进药物价格下降,使全球患者有能力负担并获得治疗。
Nephrology On-line: How do you envision the treatment paradigm for complement-mediated kidney diseases evolving in the next 5 to 10 years, and what research questions are most urgent to address?
Dr Fakhouri: This is a very excellent question, because I think we are living in very changing, moving times and complement inhibitors will find their place in different indications. For example, I see in the future that C5 inhibitors will replace corticosteroids sooner or later as anti-inflammatory drugs in inflammatory kidney disease. This would be a great change for doctors, but especially for patients. They could be spared the side effects of corticosteroids while achieving potentially a better renal remission. The second change I see is that we are moving towards a more targeted, specific pathogenesis-based approach to disease, where if you have an alternative pathway dysregulated, you have to target the alternative pathway. So, we are moving towards a fine-tuned, precise inhibition of the complement system, not a global inhibition like we had initially with C5 inhibition. And the third trend I see is a decrease in price due to the increase in the number of drugs and companies involved in the complement field, which would be good news for patients because decrease in price would make it more affordable and more easily available for patients worldwide.
四、补体领域:下一个肾脏病学革新前沿
“两三年前,SGLT2抑制剂和GLP-1受体激动剂引领了代谢性肾病的突破;如今,补体抑制正在开启新的治疗纪元。”Fakhouri在访谈中感慨。在ERA年会的众多议题中,补体抑制专场无疑成为焦点。从基础研究到临床转化的加速,将让补体靶向治疗成为继免疫抑制剂之后的又一里程碑。
Nephrology On-line: You have probably given a lot of talks, also joined a lot of sessions. Have you seen any sessions that you think are particularly interesting?
Dr Fakhouri: I think the complement inhibition is making a great revolution. Two or three years ago, we had the SGLT2 inhibitors and GLP-1 receptor agonists emerging into the light, and now it is time for complement inhibition. That is why I'm very happy to be here.
总结及展望
肾脏疾病治疗的范式正发生重要变革,尤其是补体治疗领域。除Pegcetacoplan外,针对C5、C1q、H因子等靶点的抑制剂已进入不同研发阶段,形成覆盖补体全通路的治疗矩阵。这不是单一药物的胜利,而是整个领域对疾病机制深入理解的成果。随着精准医学和人工智能在生物标志物发现中的应用,补体抑制疗法将进一步个性化,为终末期肾病的预防带来希望。
未来肾脏疾病的诊断不仅要依赖肾活检,更要结合血液和尿液中的补体活化标志物,如 C3a、C5a,实现疗效的动态监测。” 此外,如何确定最佳治疗疗程、筛选能安全停药的患者,以及探索补体抑制剂与其他靶向药物的联合方案,都是亟待解决的课题。
- 推荐文章
肾例明鉴 | 老年男性ANCA相关性血管炎伴口干、眼干:只是非特异性抗体阳性?还是重叠综合征?——1例病例报告并文献综述
恩格列净+非奈利酮联用,高钾血症风险几何?CONFIDENCE试验二次分析结果揭晓
人人享有肾脏健康:关爱生命,守护地球——2026年世界肾脏日公益活动举行
14:00直播!2026年世界肾脏日公益活动即将开始——人人享有肾脏健康:关爱生命,守护地球
血液透析的环境挑战与可持续发展路径探索——2026世界肾脏日特别关注
特别策划 | 世界肾脏日:您真的了解肾脏健康吗?
肾域华章 | 儿童增殖性狼疮肾炎初始治疗添安全新选:多中心RCT证实吗替麦考酚酯非劣效于环磷酰胺选
2026世界肾脏日 | 绿色肾移植十策:让肾移植告别等待,共护双肾与地球
靶向清除“僵尸细胞”,达沙替尼联合槲皮素为糖尿病肾病治疗开辟新路径
慢性肾脏病与认知障碍:肾病越重,认知风险越高?——基于CRIC研究的新发现
膜性肾病精准诊疗的新证据:生物标志物和临床病理特征研究进展
eGFR百分位数:CKD早期识别的个性化新工具
PI解读:FSGS治疗新曙光——靶向药物迎来突破性进展
突破性进展:靶向补体因子B的RNA疗法为IgA肾病治疗带来新希望
利妥昔单抗血药浓度:膜性肾病早期治疗反应的预测标志物
肾例明鉴|43岁男子双下肢水肿、肌酐飙升,背后竟是两种肾病罕见叠加作祟!膜性肾病合并抗GBM病该如何破局?
Richard Lafayette教授:新型补体抑制剂时代下荚膜菌感染的防控指南
孙英贤教授牵头多中心研究:CRHCP事后分析揭秘CKM综合征不同分期强化降压价值
肾识百科|娃的肾病竟是遗传的?6种遗传性肾病家长必知!
护肾先护肠?1.2万人的迄今最大研究发现:肠道菌群及其代谢产物参与肾功能早期变化
肥胖与慢性肾脏病:不可忽视的“代谢多米诺”
《柳叶刀》:TRPC6抑制剂BI 764198治疗FSGS的Ⅱ期临床试验取得积极结果,为其足细胞靶向治疗提供首个有效证据
长期血透别忽视疼痛!平均8个部位受累,84%病程超1年、75%每日受折磨,肌肉骨骼和神经病理性痛为主要类型
近16万人数据:这样吃,大脑更年轻
美国麻省总医院最新综述:CKD-aP的诊疗进展与未来方向
超88%患者未获诊疗!Ⅲ期研究首证中国血透CKD-aP人群可从Difelikefalin治疗中获益
睡不好,血糖更难控?最新研究揭示:睡眠障碍正在悄悄扰乱你的“升糖”与“降糖”激素!
KDIGO肾小球疾病指南工作组主席Jürgen Floege教授:补体旁路途径是驱动CMKDs肾小球炎症的核心引擎
沉默的神偷!无声无息偷走小孩子肾脏功能的遗传性肾病——Dent病
国际组织在行动:CKM综合征、新型超级专科与“关爱肾脏”倡议
白蛋白尿——盐皮质激素受体拮抗剂带来肾脏获益的核心驱动因素
补体靶向时代:IgA肾病新疗法的疗效排名与精准化探索
从认知到实践:中国肾脏科医生IgA肾病诊疗现状与差距
肾例明鉴丨年轻痛风不是小事!19岁小伙关节痛3年,没控尿酸把肾“熬”成慢性肾病Ⅲ期
尿酸与非酒精性脂肪肝的“隐秘关联”:高血压人群需警惕的代谢信号
狼疮肾炎患者妊娠:她安然度过,她产后风暴骤起——来自两个临床病例研究的启示
罕见的先天性肾脏发育不良疾病——肾小球巨大而又稀少的“寡巨肾”,你听说过吗?
阿塞西普:IgA肾病治疗的新曙光——ORIGIN 3试验中期数据深度剖析
生殖史如何塑造年轻女性的心肾代谢风险?
指南共识丨《IgA肾病临床实践60问(2026版)》核心要点与临床实践解读(附原文)
司美格鲁肽获批治疗2型糖尿病合并慢性肾脏病1周年:糖尿病、肾脏与心脏疾病领域的变革
佳节健康“喝”出来——咖啡与茶,提神背后的健康双面性
春节期间重磅新闻速递:膜性肾病、IgA肾病、卵巢功能早衰领域迎来治疗新进展
“钾”在悄悄溜走,肾脏在喊“救命”!一种罕见的遗传性失盐性肾小管疾病
冬季假期真的会“悄悄让人发胖”吗?
肾友过年“四大护法”!作息·出行·娱乐·情绪,这份春节健康手册请收好
新春护肾,安心团圆:肾友及四高人群春节健康全攻略
学术纵横|多维靶向,精准护肾:小干扰RNA、ASI、nsMRA、GLP-1RA等新型药物均可为CKD患者保驾护航
尿糖阳性=糖尿病?那可不一定!这种罕见肾病会遗传尿糖,别当成普通糖尿病来治
聚焦CKM综合管理,恒格列净相关复方制剂赋能心-肾-代谢多重获益
年度盘点丨周晓玲教授:肥胖相关慢性肾脏病的诊治进展
肾例明鉴丨服药后肺肾接连“报警”!20岁女生的惊魂经历:元凶竟是治疗甲亢的丙硫氧嘧啶
谨慎“跟风养生”!Omega-3、生酮饮食、禁糖等营养宣传需辩证对待
肾识百科丨肾友想生娃?4类可怀情况 + 3类禁忌,提前看清不踩坑
警惕身体的“代谢紊乱风暴”!代谢综合征——引人关注的肾脏“杀手”