
- 首页 > 正文
诺兰多西呱惊艳亮相,CKD残余风险迎来“终结者”?——ERA前主席解读心肾疾病管理方向
发表时间:2026-07-05 12:24:22
编者按:ERA前主席、德国维尔茨堡大学医院Christoph Wanner教授的主要研究方向为糖尿病肾病及其他罕见肾病患者的代谢紊乱与心血管不良结局。在2026年欧洲肾脏病学会(ERA)年会上,Christoph Wanner教授带来多项重要学术汇报,同时担任“重磅最新临床研究Ⅱ”专场主席。肾医线特邀Wanner教授围绕心肾交互机制、新型靶向药物研发、前沿临床试验成果、肾脏病患者疫苗接种四大方向展开探讨,完整梳理心肾代谢疾病领域的诊疗变革与肾脏病领域临床发展趋势。本文整理访谈要点,以飨读者。
一、心肾代谢概念成型,跨学科诊疗成为临床主流
Christoph Wanner教授指出,医学界很早就明确心脏与肾脏紧密关联,两类器官存在大量共通的致病通路。近年来心血管领域学者牵头推动学科革新,提出并完善了心肾代谢疾病(CRM)这一概念,彻底重塑了该领域研究格局。
如今心内科与肾内科跨专业协作日趋常态化,针对心、肾共病患者,临床已形成统一的一体化治疗方案。也正因心肾交互机制对慢病管理至关重要,该议题不仅是本届ERA年会的重点内容,未来一至两年仍会是全球肾脏病、心血管领域的核心研究方向。
Nephrology on-line: At ERA 2026, you are presenting on "Mechanistic Insights into the Cardio-Renal Link: Inflammation, Fibrosis and Cardiovascular Risk". From your perspective, how has our understanding of the cardio-renal connection evolved in recent years, and which mechanisms are now considered the most important therapeutic targets?
Prof. Wanner: We have known for a long time that the kidney and the heart are closely connected and share common underlying pathogenic pathways.
This field is now being reshaped through initiatives led by cardiologists. They coined the term “cardio-kidney-metabolic” or “cardio-renal-metabolic (CRM)” disease, which is now much better defined.
We are increasingly working together across specialties, and we now share common treatment strategies for both kidney and heart diseases.
That is why this topic is so important at this congress and why it will remain a major focus over the next one or two years.
二、可溶性鸟苷酸环化酶激动剂:努兰多西呱(nurandociguat)有望填补CKD治疗残余风险
Wanner教授在ERA 2026上公布了努兰多西呱治疗慢性肾脏病(CKD)的Ⅱ期临床研究数据(详细摘要数据见文末研究链接)。该药物属于可溶性鸟苷酸环化酶激动剂,作用靶点为一氧化氮-环磷酸鸟苷通路。
同通路药物已有成熟临床应用:维利西呱已获批上市用于心力衰竭治疗,后续研发管线相继推出鲁卡西呱,努兰多西呱是该靶点最新一代候选药物。
Wanner教授介绍,本次Ⅱ期试验纳入近700例慢性肾脏病患者,结果显示药物可平均降低约20%白蛋白尿。
Wanner教授表示,期待该药顺利开展大样本Ⅲ期临床试验,招募数千名受试者进一步验证疗效,证实其能够延缓肾功能持续减退,解决现有标准治疗后仍持续存在的肾脏进展与心血管残余风险。
Nephrology on-line: You are also presenting the Phase 2 trial evaluating nurandociguat in patients with CKD. Could you explain the rationale for targeting the soluble guanylate cyclase pathway in CKD, and what potential role this mechanism may play in reducing albuminuria and cardiovascular risk?
Prof. Wanner: You are asking about soluble guanylate cyclase activators, which stimulate the nitric oxide–cyclic GMP pathway.
Vericiguat is a molecule that is already on the market for the treatment of heart failure.
Then we moved to runcaciguat, and now we are evaluating nurandociguat, which is the latest molecule in this class.
It decreases albuminuria by approximately 20% on average. We tested it in about 700 patients in a Phase 2 trial.
I hope that this molecule will now be further developed in Phase 3 trials involving thousands of patients, demonstrating a slowing of CKD progression and helping to address the residual risk that remains despite current therapies.
三、ERA年会汇聚顶级循证研究,多款肾病靶向疗法迎来临床突破
作为本届年会“重磅最新临床研究Ⅱ”专场的主持专家,Wanner教授评价,ERA年会是全球随机对照试验成果的核心发布平台,被誉为肾脏病临床研究领域的“奥斯卡”盛会。Wanner教授指出,随机分组可保障均衡分组、产出高质量循证医学证据,因此,唯有随机对照试验能够客观证实一种疗法的临床获益与使用局限。
2026年大会公布了多项足以改变临床实践的关键研究,其中包括非奈利酮拓展用于非糖尿病肾病患者的相关临床试验,也包括奥法木单抗、利妥昔单抗等B细胞调节制剂应用于膜性肾病、肾病综合征的疗效探索。上述多项研究成果均刊发于《新英格兰医学杂志》《柳叶刀》《美国医学会杂志》等国际顶级医学期刊。其主持的这场重磅临床研究是本届年会最高规格环节,线下参会学者约3000人,充分体现了行业对前沿临床证据的高度重视。
Nephrology on-line: As Chair of the "Late Breaking Clinical Trials 2" session, you will be reviewing some of the latest advances in nephrology. Which emerging therapeutic areas or trial results presented at ERA 2026 do you believe could have the greatest impact on future CKD management?
Prof. Wanner: The best randomized controlled trials are presented at ERA, and ERA has become the “Oscar” of late-breaking clinical trials.
Only randomized controlled trials can truly demonstrate the benefits—or the limitations—of a treatment. Randomization makes the groups comparable and provides robust evidence.
This year, we had a number of important studies, including trials with finerenone in non-diabetic kidney disease.
We also saw studies evaluating B-cell-modulating therapies such as obinutuzumab and rituximab in patients with nephrotic syndrome and membranous nephropathy.
These randomized controlled trials have been published in leading journals such as The New England Journal of Medicine, The Lancet, and JAMA.
The Late Breaking Clinical Trials session that I chaired represents the highest-level scientific session of the congress. Today, it attracted approximately 3,000 attendees.
四、CKD人群疫苗接种亟待规范化,需纳入日常慢病管理体系
对Wanner教授的专访同时关注了慢性肾脏病患者感染防控短板。肾功能受损患者免疫力低下,带状疱疹、呼吸道合胞病毒(RSV)感染、肺炎等疾病风险显著升高,但国内及全球范围内该群体疫苗整体接种率普遍偏低。
谈及阻碍慢性肾脏病人群规范接种疫苗的核心难点,Wanner教授指出,“首要问题在于临床医师对患者疫苗接种状态关注度不足”,未将疫苗接种纳入常规评估。“肾内科已有二十余年成熟的乙肝疫苗接种流程,但对其他传染病疫苗的重视程度严重不足”。新冠疫情直观印证了疫苗对肾脏病患者远期预后的保护价值,在他看来,“规范接种疫苗对改善患者长期结局的作用,甚至优于新增一种口服治疗药物”。
他倡议所有肾内科诊疗中心组建医护协作团队,搭建系统化、全覆盖的疫苗管理流程,将疫苗筛查、接种、随访纳入慢性肾脏病标准化慢性病照护。
Nephrology on-line: Another important topic in your program is improving vaccination processes in patients with CKD. Patients with kidney disease remain highly vulnerable to infections, yet vaccination rates are often suboptimal. In your opinion, what are the major barriers to effective vaccination implementation in CKD populations, and how can nephrologists improve this aspect of patient care?
Prof. Wanner: You are asking about the major barriers.
The main problem is that we do not focus enough on the vaccination status of our patients.
Meanwhile, this vulnerable population faces increasing risks from diseases such as herpes zoster, respiratory syncytial virus (RSV) infection, and pneumonia.
Nephrologists are very familiar with hepatitis B vaccination because we have been doing it for more than 20 years. However, we have not been equally focused on vaccinations for other infectious diseases.
The COVID-19 pandemic clearly demonstrated how important vaccination is.
In fact, vaccination may have a greater impact on patient outcomes than adding yet another pill. That is my impression.
Therefore, I strongly support comprehensive vaccination programs, which should be systematically organized within every nephrology practice through a team-based approach.
结语
Wanner教授结合ERA 2026最新研究成果,勾勒出心肾代谢疾病及肾脏病未来诊疗发展路径,为全球肾内科临床工作提供了实践指引。
研究链接
努兰多西呱对慢性肾脏病患者白蛋白尿的作用:一项Ⅱ期随机剂量探索临床试验
在标准治疗基础上加用可溶性鸟苷酸环化酶(sGC)激动剂,或可成为进一步降低慢性肾脏病(CKD)患者白蛋白尿的全新方案。本试验旨在评估可溶性鸟苷酸环化酶激动剂努兰多西呱(试验代号BAY3283142)联合标准治疗,用于合并/不合并糖尿病慢性肾脏病患者的剂量-效应关系及不同口服剂量的安全性。
入组标准:估算肾小球滤过率(eGFR)20~75 ml/(min·1.73m2),尿白蛋白/肌酐比值(UACR)≥200且<3500 mg/g。
研究方法
本研究为多中心、随机、双盲、安慰剂对照剂量探索试验(临床试验注册号:NCT06522997),在全球15个国家开展。2024年8月至2025年11月于149家中心招募受试者;共筛选1222例患者,751例完成随机分组。研究设计见图1。
受试者每日口服对应药物,持续16周,停药后随访30天评估安全性:
努兰多西呱2.5 mg组(n=126);
努兰多西呱5 mg组(n=124);
努兰多西呱10 mg组(n=126);
努兰多西呱15 mg组(n=124);
努兰多西呱20 mg组(n=126);
匹配安慰剂组(n=125)。
主要疗效终点:第16周尿白蛋白/肌酐比值(UACR)对数较基线的变化;采用多重比较程序-建模法(MCP-MOD)分析剂量-效应关系。
次要疗效终点:第6、10、16周UACR对数、eGFR较基线变化,通过重复测量混合效应模型(MMRM)分析。
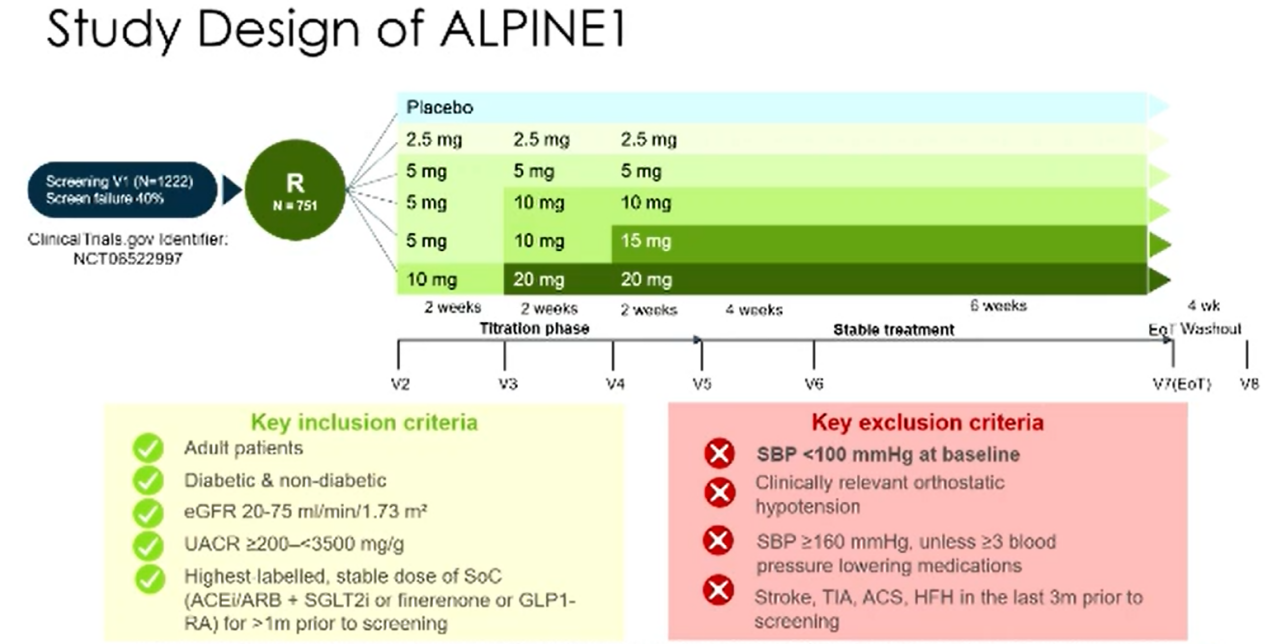
图1. 研究设计
受试者平均年龄62.5±12.3岁;男性占77%,61%合并糖尿病。基线平均血压135/79 mmHg,eGFR均值42±15.3 ml/(min·1.73m²),UACR中位数650 mg/g(四分位距378~1218 mg/g)。
基线治疗情况:96.3%患者使用血管紧张素转换酶抑制剂(ACEI)/血管紧张素受体拮抗剂(ARB);69.6%使用钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i);23.2%使用盐皮质激素受体拮抗剂。
主要终点:各组存在具有统计学意义的剂量-效应关系。
第16周UACR最小二乘几何均值比值(95%置信区间):
安慰剂组1.10(0.86,1.40);2.5 mg组0.86(0.68,1.09);5 mg组0.92(0.73,1.18);10 mg组0.79(0.62,1.01);15 mg组0.89(0.70,1.14);20 mg组0.87(0.69,1.11)。
校正安慰剂效应后的UACR几何均值比值(预设次要终点,MMRM模型):全部努兰多西呱剂量组UACR均较基线下降:2.5 mg组0.79(0.67,0.93);5 mg组0.84(0.71,0.99);10 mg组0.72(0.61,0.86);15 mg组0.81(0.68,0.96);20 mg组0.80(0.68,0.95)。图2可见各剂量组校正安慰剂后UACR均呈下降趋势。
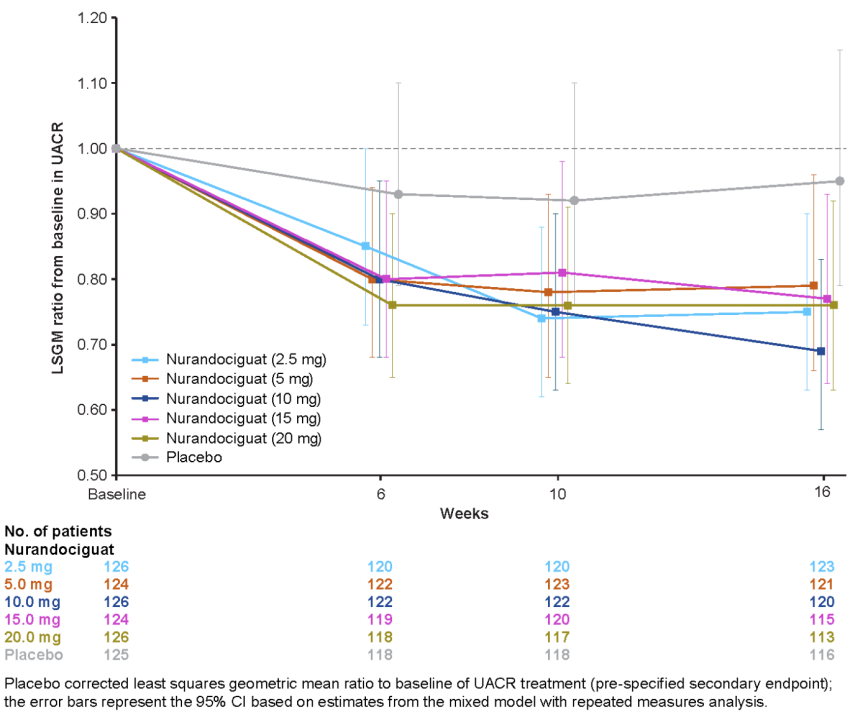
图2. 预设次要终点
(引自大会摘要132)
肾功能指标:16周内,各努兰多西呱剂量组与安慰剂组相比,eGFR无具有临床意义的差异。
安全性:努兰多西呱整体组治疗期间不良事件发生率63.3%,安慰剂组52.8%。
重点关注不良事件——症状性低血压:全部努兰多西呱合并组发生率10.7%;其中2.5 mg组5.6%、5 mg组5.6%、10 mg组10.3%、15 mg组11.3%、20 mg组20.6%;安慰剂组仅1.6%。
结论
本研究纳入的慢性肾脏病患者绝大多数基线已接受ACEI/ARB联合SGLT2i标准治疗,在此基础上加用可溶性鸟苷酸环化酶激动剂努兰多西呱,可使患者尿白蛋白/肌酐比值下降20%~30%,且不会对eGFR产生急性影响。仍需开展后续临床试验,进一步探究努兰多西呱对肾脏终点及心血管终点事件的长期获益。
一、心肾代谢概念成型,跨学科诊疗成为临床主流
Christoph Wanner教授指出,医学界很早就明确心脏与肾脏紧密关联,两类器官存在大量共通的致病通路。近年来心血管领域学者牵头推动学科革新,提出并完善了心肾代谢疾病(CRM)这一概念,彻底重塑了该领域研究格局。
如今心内科与肾内科跨专业协作日趋常态化,针对心、肾共病患者,临床已形成统一的一体化治疗方案。也正因心肾交互机制对慢病管理至关重要,该议题不仅是本届ERA年会的重点内容,未来一至两年仍会是全球肾脏病、心血管领域的核心研究方向。
Nephrology on-line: At ERA 2026, you are presenting on "Mechanistic Insights into the Cardio-Renal Link: Inflammation, Fibrosis and Cardiovascular Risk". From your perspective, how has our understanding of the cardio-renal connection evolved in recent years, and which mechanisms are now considered the most important therapeutic targets?
Prof. Wanner: We have known for a long time that the kidney and the heart are closely connected and share common underlying pathogenic pathways.
This field is now being reshaped through initiatives led by cardiologists. They coined the term “cardio-kidney-metabolic” or “cardio-renal-metabolic (CRM)” disease, which is now much better defined.
We are increasingly working together across specialties, and we now share common treatment strategies for both kidney and heart diseases.
That is why this topic is so important at this congress and why it will remain a major focus over the next one or two years.
二、可溶性鸟苷酸环化酶激动剂:努兰多西呱(nurandociguat)有望填补CKD治疗残余风险
Wanner教授在ERA 2026上公布了努兰多西呱治疗慢性肾脏病(CKD)的Ⅱ期临床研究数据(详细摘要数据见文末研究链接)。该药物属于可溶性鸟苷酸环化酶激动剂,作用靶点为一氧化氮-环磷酸鸟苷通路。
同通路药物已有成熟临床应用:维利西呱已获批上市用于心力衰竭治疗,后续研发管线相继推出鲁卡西呱,努兰多西呱是该靶点最新一代候选药物。
Wanner教授介绍,本次Ⅱ期试验纳入近700例慢性肾脏病患者,结果显示药物可平均降低约20%白蛋白尿。
Wanner教授表示,期待该药顺利开展大样本Ⅲ期临床试验,招募数千名受试者进一步验证疗效,证实其能够延缓肾功能持续减退,解决现有标准治疗后仍持续存在的肾脏进展与心血管残余风险。
Nephrology on-line: You are also presenting the Phase 2 trial evaluating nurandociguat in patients with CKD. Could you explain the rationale for targeting the soluble guanylate cyclase pathway in CKD, and what potential role this mechanism may play in reducing albuminuria and cardiovascular risk?
Prof. Wanner: You are asking about soluble guanylate cyclase activators, which stimulate the nitric oxide–cyclic GMP pathway.
Vericiguat is a molecule that is already on the market for the treatment of heart failure.
Then we moved to runcaciguat, and now we are evaluating nurandociguat, which is the latest molecule in this class.
It decreases albuminuria by approximately 20% on average. We tested it in about 700 patients in a Phase 2 trial.
I hope that this molecule will now be further developed in Phase 3 trials involving thousands of patients, demonstrating a slowing of CKD progression and helping to address the residual risk that remains despite current therapies.
三、ERA年会汇聚顶级循证研究,多款肾病靶向疗法迎来临床突破
作为本届年会“重磅最新临床研究Ⅱ”专场的主持专家,Wanner教授评价,ERA年会是全球随机对照试验成果的核心发布平台,被誉为肾脏病临床研究领域的“奥斯卡”盛会。Wanner教授指出,随机分组可保障均衡分组、产出高质量循证医学证据,因此,唯有随机对照试验能够客观证实一种疗法的临床获益与使用局限。
2026年大会公布了多项足以改变临床实践的关键研究,其中包括非奈利酮拓展用于非糖尿病肾病患者的相关临床试验,也包括奥法木单抗、利妥昔单抗等B细胞调节制剂应用于膜性肾病、肾病综合征的疗效探索。上述多项研究成果均刊发于《新英格兰医学杂志》《柳叶刀》《美国医学会杂志》等国际顶级医学期刊。其主持的这场重磅临床研究是本届年会最高规格环节,线下参会学者约3000人,充分体现了行业对前沿临床证据的高度重视。
Nephrology on-line: As Chair of the "Late Breaking Clinical Trials 2" session, you will be reviewing some of the latest advances in nephrology. Which emerging therapeutic areas or trial results presented at ERA 2026 do you believe could have the greatest impact on future CKD management?
Prof. Wanner: The best randomized controlled trials are presented at ERA, and ERA has become the “Oscar” of late-breaking clinical trials.
Only randomized controlled trials can truly demonstrate the benefits—or the limitations—of a treatment. Randomization makes the groups comparable and provides robust evidence.
This year, we had a number of important studies, including trials with finerenone in non-diabetic kidney disease.
We also saw studies evaluating B-cell-modulating therapies such as obinutuzumab and rituximab in patients with nephrotic syndrome and membranous nephropathy.
These randomized controlled trials have been published in leading journals such as The New England Journal of Medicine, The Lancet, and JAMA.
The Late Breaking Clinical Trials session that I chaired represents the highest-level scientific session of the congress. Today, it attracted approximately 3,000 attendees.
四、CKD人群疫苗接种亟待规范化,需纳入日常慢病管理体系
对Wanner教授的专访同时关注了慢性肾脏病患者感染防控短板。肾功能受损患者免疫力低下,带状疱疹、呼吸道合胞病毒(RSV)感染、肺炎等疾病风险显著升高,但国内及全球范围内该群体疫苗整体接种率普遍偏低。
谈及阻碍慢性肾脏病人群规范接种疫苗的核心难点,Wanner教授指出,“首要问题在于临床医师对患者疫苗接种状态关注度不足”,未将疫苗接种纳入常规评估。“肾内科已有二十余年成熟的乙肝疫苗接种流程,但对其他传染病疫苗的重视程度严重不足”。新冠疫情直观印证了疫苗对肾脏病患者远期预后的保护价值,在他看来,“规范接种疫苗对改善患者长期结局的作用,甚至优于新增一种口服治疗药物”。
他倡议所有肾内科诊疗中心组建医护协作团队,搭建系统化、全覆盖的疫苗管理流程,将疫苗筛查、接种、随访纳入慢性肾脏病标准化慢性病照护。
Nephrology on-line: Another important topic in your program is improving vaccination processes in patients with CKD. Patients with kidney disease remain highly vulnerable to infections, yet vaccination rates are often suboptimal. In your opinion, what are the major barriers to effective vaccination implementation in CKD populations, and how can nephrologists improve this aspect of patient care?
Prof. Wanner: You are asking about the major barriers.
The main problem is that we do not focus enough on the vaccination status of our patients.
Meanwhile, this vulnerable population faces increasing risks from diseases such as herpes zoster, respiratory syncytial virus (RSV) infection, and pneumonia.
Nephrologists are very familiar with hepatitis B vaccination because we have been doing it for more than 20 years. However, we have not been equally focused on vaccinations for other infectious diseases.
The COVID-19 pandemic clearly demonstrated how important vaccination is.
In fact, vaccination may have a greater impact on patient outcomes than adding yet another pill. That is my impression.
Therefore, I strongly support comprehensive vaccination programs, which should be systematically organized within every nephrology practice through a team-based approach.
结语
Wanner教授结合ERA 2026最新研究成果,勾勒出心肾代谢疾病及肾脏病未来诊疗发展路径,为全球肾内科临床工作提供了实践指引。
研究链接
努兰多西呱对慢性肾脏病患者白蛋白尿的作用:一项Ⅱ期随机剂量探索临床试验
在标准治疗基础上加用可溶性鸟苷酸环化酶(sGC)激动剂,或可成为进一步降低慢性肾脏病(CKD)患者白蛋白尿的全新方案。本试验旨在评估可溶性鸟苷酸环化酶激动剂努兰多西呱(试验代号BAY3283142)联合标准治疗,用于合并/不合并糖尿病慢性肾脏病患者的剂量-效应关系及不同口服剂量的安全性。
入组标准:估算肾小球滤过率(eGFR)20~75 ml/(min·1.73m2),尿白蛋白/肌酐比值(UACR)≥200且<3500 mg/g。
研究方法
本研究为多中心、随机、双盲、安慰剂对照剂量探索试验(临床试验注册号:NCT06522997),在全球15个国家开展。2024年8月至2025年11月于149家中心招募受试者;共筛选1222例患者,751例完成随机分组。研究设计见图1。
受试者每日口服对应药物,持续16周,停药后随访30天评估安全性:
努兰多西呱2.5 mg组(n=126);
努兰多西呱5 mg组(n=124);
努兰多西呱10 mg组(n=126);
努兰多西呱15 mg组(n=124);
努兰多西呱20 mg组(n=126);
匹配安慰剂组(n=125)。
主要疗效终点:第16周尿白蛋白/肌酐比值(UACR)对数较基线的变化;采用多重比较程序-建模法(MCP-MOD)分析剂量-效应关系。
次要疗效终点:第6、10、16周UACR对数、eGFR较基线变化,通过重复测量混合效应模型(MMRM)分析。
图1. 研究设计
(引自讲者报告)
受试者平均年龄62.5±12.3岁;男性占77%,61%合并糖尿病。基线平均血压135/79 mmHg,eGFR均值42±15.3 ml/(min·1.73m²),UACR中位数650 mg/g(四分位距378~1218 mg/g)。
基线治疗情况:96.3%患者使用血管紧张素转换酶抑制剂(ACEI)/血管紧张素受体拮抗剂(ARB);69.6%使用钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i);23.2%使用盐皮质激素受体拮抗剂。
主要终点:各组存在具有统计学意义的剂量-效应关系。
第16周UACR最小二乘几何均值比值(95%置信区间):
安慰剂组1.10(0.86,1.40);2.5 mg组0.86(0.68,1.09);5 mg组0.92(0.73,1.18);10 mg组0.79(0.62,1.01);15 mg组0.89(0.70,1.14);20 mg组0.87(0.69,1.11)。
校正安慰剂效应后的UACR几何均值比值(预设次要终点,MMRM模型):全部努兰多西呱剂量组UACR均较基线下降:2.5 mg组0.79(0.67,0.93);5 mg组0.84(0.71,0.99);10 mg组0.72(0.61,0.86);15 mg组0.81(0.68,0.96);20 mg组0.80(0.68,0.95)。图2可见各剂量组校正安慰剂后UACR均呈下降趋势。
图2. 预设次要终点
(引自大会摘要132)
肾功能指标:16周内,各努兰多西呱剂量组与安慰剂组相比,eGFR无具有临床意义的差异。
安全性:努兰多西呱整体组治疗期间不良事件发生率63.3%,安慰剂组52.8%。
重点关注不良事件——症状性低血压:全部努兰多西呱合并组发生率10.7%;其中2.5 mg组5.6%、5 mg组5.6%、10 mg组10.3%、15 mg组11.3%、20 mg组20.6%;安慰剂组仅1.6%。
结论
本研究纳入的慢性肾脏病患者绝大多数基线已接受ACEI/ARB联合SGLT2i标准治疗,在此基础上加用可溶性鸟苷酸环化酶激动剂努兰多西呱,可使患者尿白蛋白/肌酐比值下降20%~30%,且不会对eGFR产生急性影响。仍需开展后续临床试验,进一步探究努兰多西呱对肾脏终点及心血管终点事件的长期获益。
- 推荐文章
诺兰多西呱惊艳亮相,CKD残余风险迎来“终结者”?——ERA前主席解读心肾疾病管理方向
路万虹教授:基于2026 KDIGO指南更新的肾性贫血诊疗进展
虚弱不仅是结局,更可能推动糖尿病肾病进展?
研究者解读:SGLT2抑制剂治疗Alport综合征的新证据
ERA 2026前沿 | 突破诊疗壁垒,迈向全程管理:构建以SGLT2i为核心的CKD早筛早诊早治新格局
崔兆强教授:利尿剂——高血压治疗中难以替代的“基石”与“放大器”
FDA就暂不批准碳酸氧镧治疗透析慢性肾脏病患者高磷血症的适应证发出完整回应函
CKD管理新证据:司美格鲁肽改善生活质量,阿司匹林用于心血管疾病一级预防不推荐
CKM视角下的心血管一级预防:为何司美格鲁肽被推至前沿?
靶向补体治疗免疫性肾病的临床研究进展
佟倩教授:高血压治疗,指南与临床的鸿沟如何跨越?
无尿背后的致命陷阱!肾皮质坏死,比急性肾损伤更凶险的沉默杀手
对话何志凌教授:从“降压达标”到“靶器官共护”,国产原研ARNI如何重塑高血压全生命周期管理?
肾实质性高血压诊疗路径:从机制解析到精准靶目标管理,再到药物选择的肾保护策略
高血压精准管理新动向:关注难治性高血压患者中皮质醇增多症的筛查丨ACC.26
家族里多人早发痛风?小心一种常染色体遗传病:尿调节素相关肾病会悄悄毁肾
推翻激素假说:炎症是慢性肾脏病女性生育力受损的“隐藏推手”——一项观察性蛋白质组学与遗传流行病学研究探索
双靶点协同护肾心——醛固酮合酶抑制剂联合SGLT2 抑制剂的BaxDuo系列临床研究项目稳步推进
久坐越少越好?最新研究带来新发现:每天约4小时久坐风险最低
葡萄牙学者发布初发肾病综合征患者5年肾衰竭风险预测模型
早干预、规范治、新药破局——慢性肾脏病心肾保护新策略解读
C4d沉积预警IgA肾病患者肾衰竭,凝集素通路激活提示预后不良
第二届肾小球疾病中外大咖面对面(CIG):深耕肠道黏膜靶向治疗,筑牢IgA肾病对因治疗、保护肾功能基石地位
OCN 2026丨臧秀娟教授:非透析患者HK的诊疗新进展——从隐匿诊断到精准治疗的“破局”
张宏/吕继成教授深度专访:首个中国原研SGLT2i恒格列净联合内皮素受体拮抗剂证据荣登JASN,破解临床联合用药困局
肾例明鉴丨68岁老人反复鼻塞咳血+肾功能急跌!警惕这种“伪装”成肿瘤的自身免疫病
学术纵横|“满堂亮”是IgA肾病肾小球坏死的可靠标志物,不同补体抑制剂感染风险存异
李冰教授:IgA肾病机制及治疗新进展——未来已来
【会议预热】大咖云集,共探前沿|第二届肾小球疾病中外大咖面对面(CIG)学术研讨即将启幕!
CCBPC 2026 | 梁伟教授:用药越多,疗效越差?CKD药物相互作用的临床警示
中国2026 CKM综合征评估、诊断、治疗专家共识重磅发布,CKM 0~4期管理路径尽收眼底
边波教授:从血压控制到心血管风险防控,步入高血压综合管理新时代
盘点6月肾脏领域新进展:多款新药获批+多项重磅研究数据收入囊中,学习休闲两不误
2026年度SCI影响因子正式发布,肾脏病与泌尿领域最新TOP 10期刊排名揭晓,哪些期刊成功上榜?
余静教授:高血压管理新风向——从疾病负担到精准治疗的全面革新
CCBPC丨阳晓教授:进展至无尿,腹透还值得坚持吗?
7月4日-5日 | 广东省医院协会肾脏病防治与血液净化中心管理专业委员会换届选举会议暨2026年学术年会
临床必备!2026版中国CKD筛查、诊断及治疗指南32条推荐意见、12张表格、1张流程图速览
NDT:三大国际权威指南更新对比,狼疮性肾炎迎来靶向新时代
蔡军教授:心血管病诊疗向治愈进阶、向预防前移、向舒适升级
CCBPC 2026|彭晖教授:腹膜透析影响心血管系统的多维度解析
肾科领域迎来新突破!DMX-200推进至全球Ⅲ期临床研究,FSGS治疗有望打破僵局
中国创新药的破局之作:揭秘全球第二款ARNI类药物沙库巴曲阿利沙坦的研发征程
学术纵横|血清PLA2R抗体检测存在局限性,奥妥珠单抗治疗难治性pMN疗效确切
《补体相关性肾病诊断和治疗专家共识》要点概览
UACR降幅超40%!中国迄今最大规模非奈利酮真实世界研究在ADA2026首次公布
韩飞教授:联合免疫靶向治疗急进性肾炎的临床探索与研究进展
沪上聚贤论肾道,东方盛会谱新篇——第十六届东方肾脏病学会议开幕
肾例明鉴丨隐匿在民间偏方里的肾衰陷阱!“朱砂莲”暗藏马兜铃酸剧毒,男子从服药到肾衰仅十余天
超万人注册参会、新药爆发、异种移植可期——ERA秘书长详解第63届ERA大会重磅进展
时隔4年,2026年ADA/EASD 2型糖尿病高血糖管理共识声明草案公布 | ADA2026
ERA专家访谈 | 范秋灵教授:补体抑制剂助力蛋白尿深度缓解,口服盐酸兰诺可泮治疗lgA肾病12周达标率高达40%
ERA中国之声 | 从DNA到RNA再到组蛋白——同济医院三项口头报告解码CKD血管钙化的表观遗传网络
重磅发布!首部CKM综合征管理指南全新出炉,开启慢病治疗新时代!
ERA专家访谈丨顾乐怡教授:补体相关肾病治疗格局的范式跃迁,口服盐酸兰诺可泮治疗lgA肾病12周尿蛋白达标率高达40%